3.
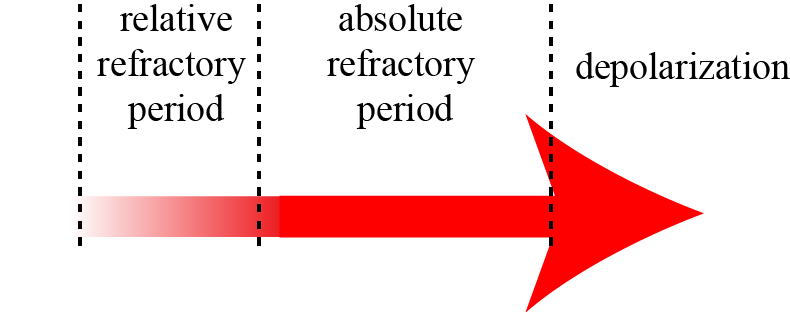
Triggered activity: Early After Depolarization:
Sometimes, during the plateau phase of the action potential, a spontaneous depolarization may occur. This is often the case when there is too much calcium in the cell. These depolarisations may reach threshold and induce, too soon, a newaction potential: