Arrhythmias are usually divided into those that occur in the ventricles and those that occur in the atrium, above the ventricles, also called “supra-ventricular”.
There are a few arrhythmias that do not fit into one of these two groups. The most famous one is the WPW syndrome (=Wolf-Parkinson-White; see panel E).
5.
Also, the duration of the arrhythmia is important.
6.
There are three types:
Paroxysmal: lasts for seconds to a few hours
Persistent: lasts for days to weeks
Chronic: lasts months to years.
Ventricular Arrhythmias
A. Atrio-ventricular block
1.
In this disease, the impulse has difficulty in propagating from the atria, through the AV-node, into the ventricles.
2.
Based on the behaviour of the heart, there are three types of AV-blocks:
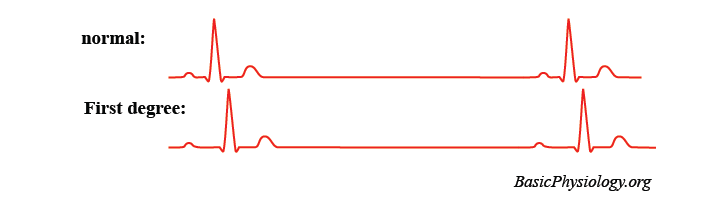
3. First degree AV-block:
This is not really a block but the impulse takes longer than normal to propagate through the AV-node. This is visible on the ECG by a longer PQ-interval.
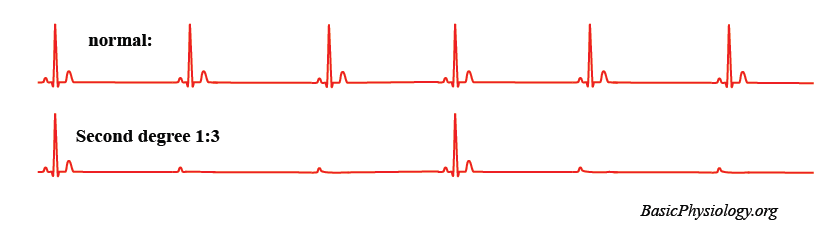
Second degree AV-block:
In this situation, some impulses propagate through the AV-node and some do not. The ratio between those that pass and those that do not pass can be expressed; for example, 1:3 second degree AV-block (as in this case).
Third degree AV-block:
In this case, there is total block between the atrium and the ventricles. The atrium will continue to function as before, visible by the P waves.
6.
The ventricles will also produce impulses (from the Purkinje system) but at a lower rate than the atrium. Furthermore, there is no relationship any more between the atrial activity (and contraction) and that of the ventricles.
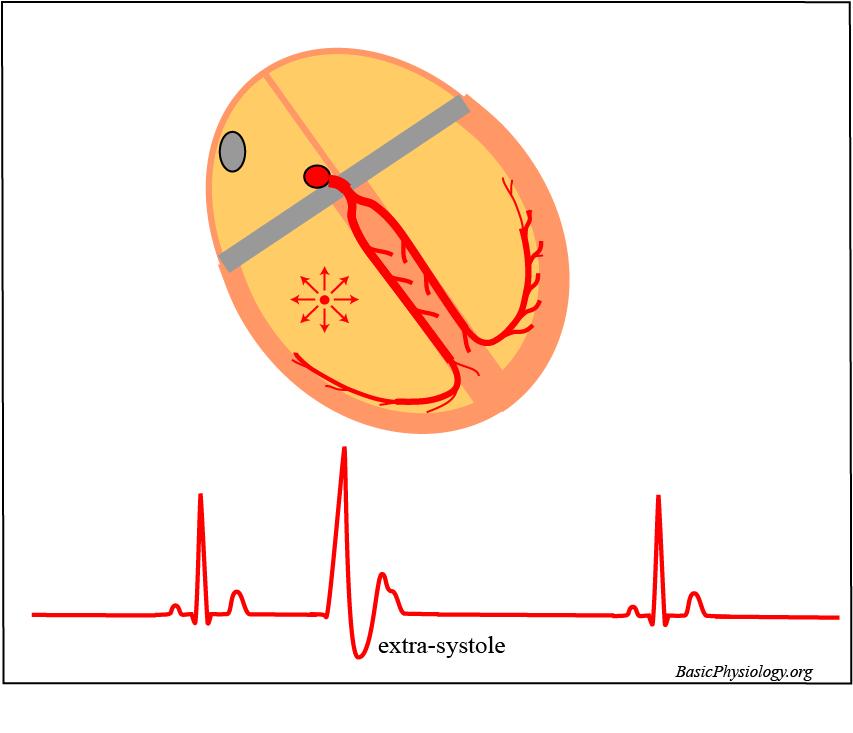
As with the atrial extra systole, the ventricular extra systole is an “extra” beat.
2.
But this time, the extra beat starts somewhere in the ventricles and not in the atria.
3.
There is therefore no relationship between the P wave and the QRS complex.
4.
In addition, and most importantly, the shape of the QRS has changed. This is because the propagation in the ventricles is different from the normal propagation.
5.
Therefore, the shape of this strange QRS can be very weird and unpredictable.
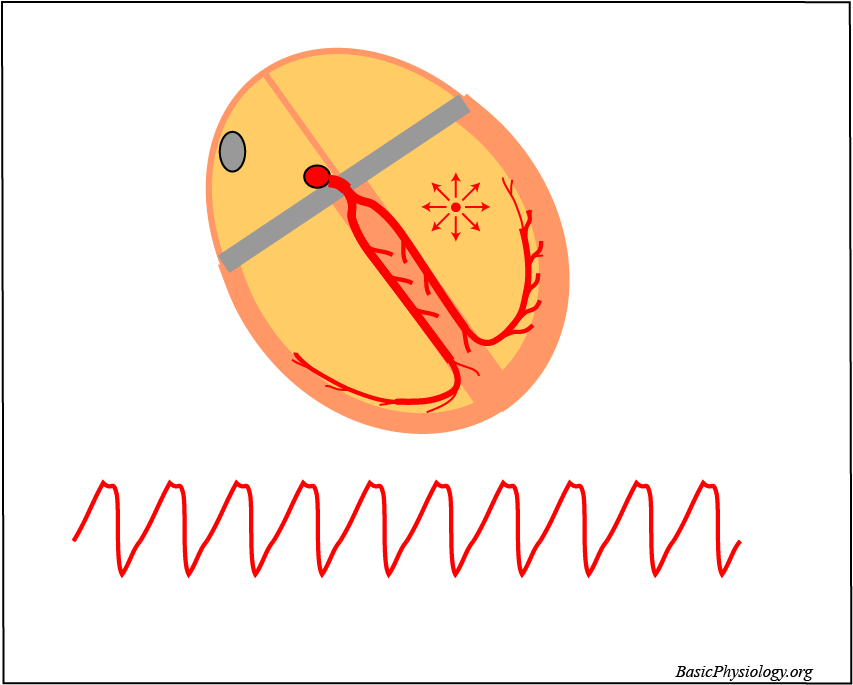
In ventricular fibrillation, there are multiple re-entrant propagations simultaneously present, in the right and in the left ventricles.
2.
Therefore, some parts of the ventricles are constantly excited while others are recovering. All these excited and recovering areas shift all the time throughout the muscle.
3.
As there is no longer one single propagating impulse, there is no longer a significant signal on the ECG and therefore no QRS and T waves.
4.
Because the heart is no longer contracting, it is not pumping any blood, and the whole heart will become very quickly hypoxic and ischemic.
5.
This will also affect the right atrium and the sinus node and the P wave will also disappear. This is the final arrhythmia!
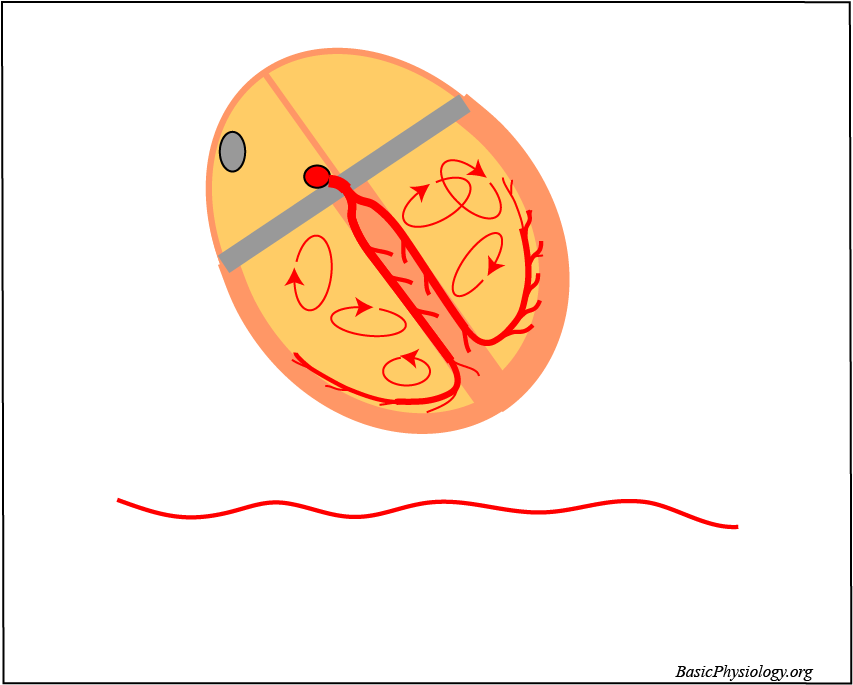
In the Wolf-Parkinson-White syndrome, the AV-bundle is not the only connection between the atria and the ventricles.
2.
In this disease, there are other muscle fibres that connect the atria to the ventricles. These fibres are often named as the bundle of Kent (after the first discoverer).
3.
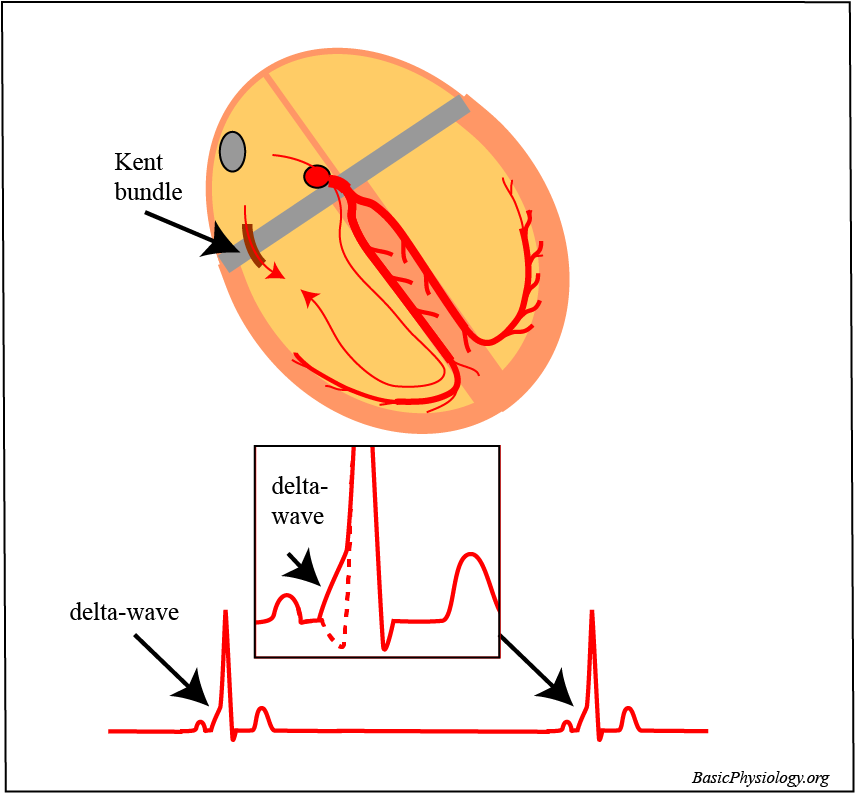
When the heart beats normally, this bundle of Kent will be visible on the ECG as a “delta-wave”.
4.
The delta wave is caused by the fact that the atrial impulse does not only activate the ventricles through the normal AV-node but now also through the bundle of Kent.
5.
Because the Kent bundle does not delay the impulse (as the AV-node does), the ventricles will be activated a bit earlier than normal. Therefore, the PQ-time will be shorter than normal.
6.
In addition, because this earlier activation is propagating more slowly through the ventricle than through the Purkinje system, the delta wave is a slow wave on the ECG.
7.
However, the impulse also propagates through the AV-node and, after this delay, is conducted rapidly through the Purkinje system. This conduction is much faster than the impulse through the Kent bundle. Therefore, the major and second part of the QRS shows a normal configuration.
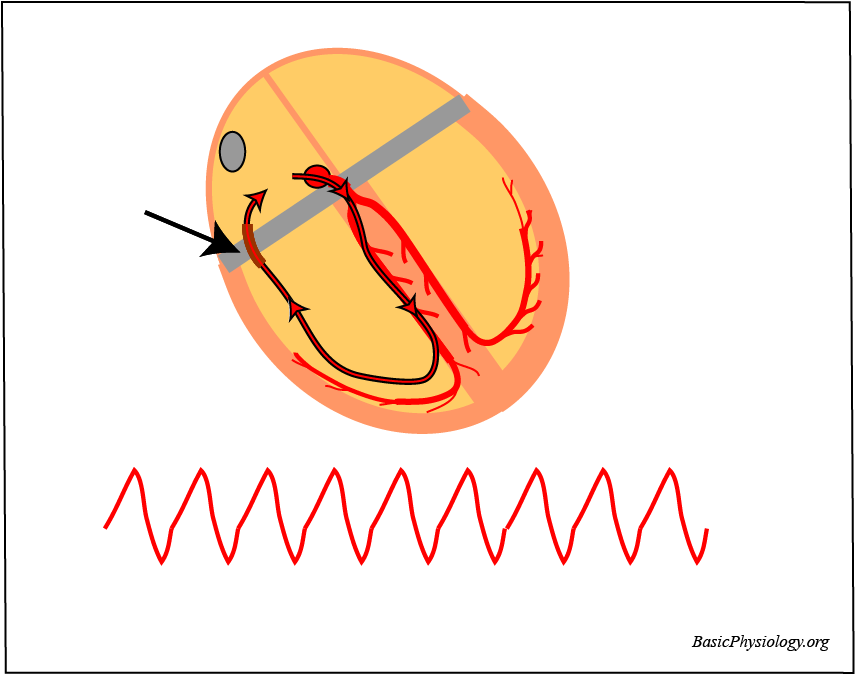
Patients who suffer from the presence of such an abnormal AV-bundle often complain of sudden (paroxysmal) palpitations.
2.
In that situation, the heart is beating much faster than normal. This is therefore a tachycardia.
3.
What is happening is shown in the diagram. An impulse is now propagating from the right atrium, through the AV-node and Purkinje system to the ventricles and conducting back into the right atrium through the bundle of Kent.
4.
Therefore, this impulse is continuously propagating in a large re-entrant loop: from atria to ventricles to atria to ventricles etc etc.
5.
This abnormal rhythm is often called a “reciprocating rhythm” because the impulse is continuously “reciprocating” or propagating between the atria and the ventricles.
6.
For the ECG, it looks very much like a ventricular tachycardia.
7.
This rhythm is uncomfortable for the patient but does not kill. However, there is now another situation possible that will certainly kill the patient.
8.
If for some reason the atria fibrillate then the situation becomes very dangerous. Then, all the impulses can propagate through the bundle of Kent to the ventricles. All these impulses will then make the ventricles fibrillate, which will immediately kill the patient. This is a typical example of “suddendeath”.
9.
Note that this does not happen in a normal heart. There, if the atria fibrillate, most impulses from the fibrillating atria will not reach the ventricles as they are delayed and blocked by the AV-node.
10.
Therefore, in the normal heart, the AV-node protects the ventricles. But in WPW patients, their ventricles are not protected due to the presence of the abnormal Kent-bundles.