3.
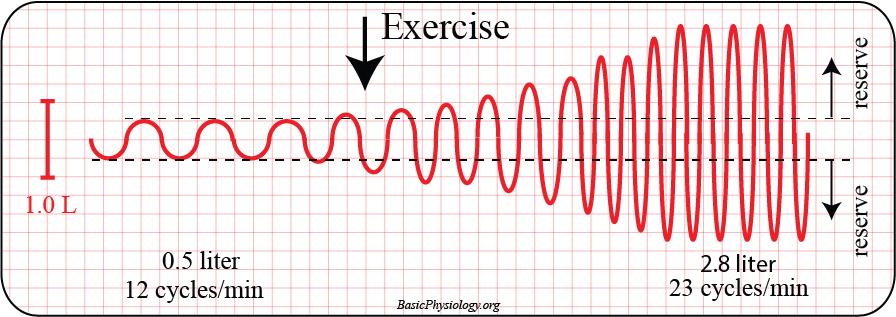
We call the volume that is in- and expired the tidal volume (= from ‘tide’; going in and out, like the sea tide at the beach).
The tidal volume is, at rest, typically about 500 ml (= half a liter!).
The frequency of respiration, again at rest, is typically 12 cpm (cycles per min).





{kind=link}